Compensation Patterns
Hello everybody!
Today I’d like to talk about compensation patterns. When I was in school, I learned the basics about muscular compensation. I knew the simple idea that if one muscle wasn’t going to do its job, another muscle would pick up the slack. I thought I had a decent grasp on the concept, especially when you match up muscular compensation with something like lower cross syndrome. It wasn’t until recently that I put together multiple pieces of the puzzle to better understand how compensation works.
I have previously mentioned Douglas Heel’s body zones and Tom Myers’ anatomy trains as key
 components in describing compensation patterns. Myers sets the tone with his understanding of how the body is connected through a complex fascial system and how force easily travels from one area to another. More recently I have received my level 1 Reflexive Performance Reset (RPR) certification. RPR is partially based on Heel’s Be Activated course, specifically one element that carries over is the depiction of the body using three zones to create a target-like image with zone 1 at the center. The zones of the body help to visualize how power is generated during movement. Ideally movement will be generated from zone 1 and move out to zone 3, acting almost like a whip where the handle would be zone 1 and the end of the whip is zone 3. It’s impossible to crack a whip when holding the end instead of the handle, i.e. power production is significantly reduced when zone 3 works before zone 1 or 2.
components in describing compensation patterns. Myers sets the tone with his understanding of how the body is connected through a complex fascial system and how force easily travels from one area to another. More recently I have received my level 1 Reflexive Performance Reset (RPR) certification. RPR is partially based on Heel’s Be Activated course, specifically one element that carries over is the depiction of the body using three zones to create a target-like image with zone 1 at the center. The zones of the body help to visualize how power is generated during movement. Ideally movement will be generated from zone 1 and move out to zone 3, acting almost like a whip where the handle would be zone 1 and the end of the whip is zone 3. It’s impossible to crack a whip when holding the end instead of the handle, i.e. power production is significantly reduced when zone 3 works before zone 1 or 2.

From Myers’ work, it is easy to assimilate the body to a single strand of string where everything is connected and force on one end can translate to an effect on the other end. Then I superimposed Heel’s zones onto the string where zone 1 is the middle, zone 2 is on either side of 1 and zone 3 is either end of the string. This would be the same layout if the target image of the zones were on a person laying down. Now that we have combined the two approaches we can discuss how compensation patterns exist. Let’s consider the movement of a supine hip thrust, a.k.a. a glute bridge. Ideally that movement is generated by the glutes with the goal of lifting zone 1 off the table/floor. The body always finds a way to move and to breathe, so if the glutes will not or cannot complete the movement then the body will achieve the goal of lifting the hips off the table through activation of zone 2 and/or 3. Imagine a string lying straight on the surface in front of you. If you pinch your fingers and pick up the string in zone 1, that would be the same as a glute bridge. Now if you were to pinch either end of the string and lift until zone 1 came off the surface, this would be a compensation. I created an image seen below to help demonstrate what I’m describing. Please note, picking up the string is not a direct model of a glute bridge, I am not suggesting that lifting one’s arms in zone 3 will lift the hips off the table, though tension generated on one end of the kinetic chain can cause an effect at the other end. It is merely a representation of how compensation works in regards to force production in the three body zones.
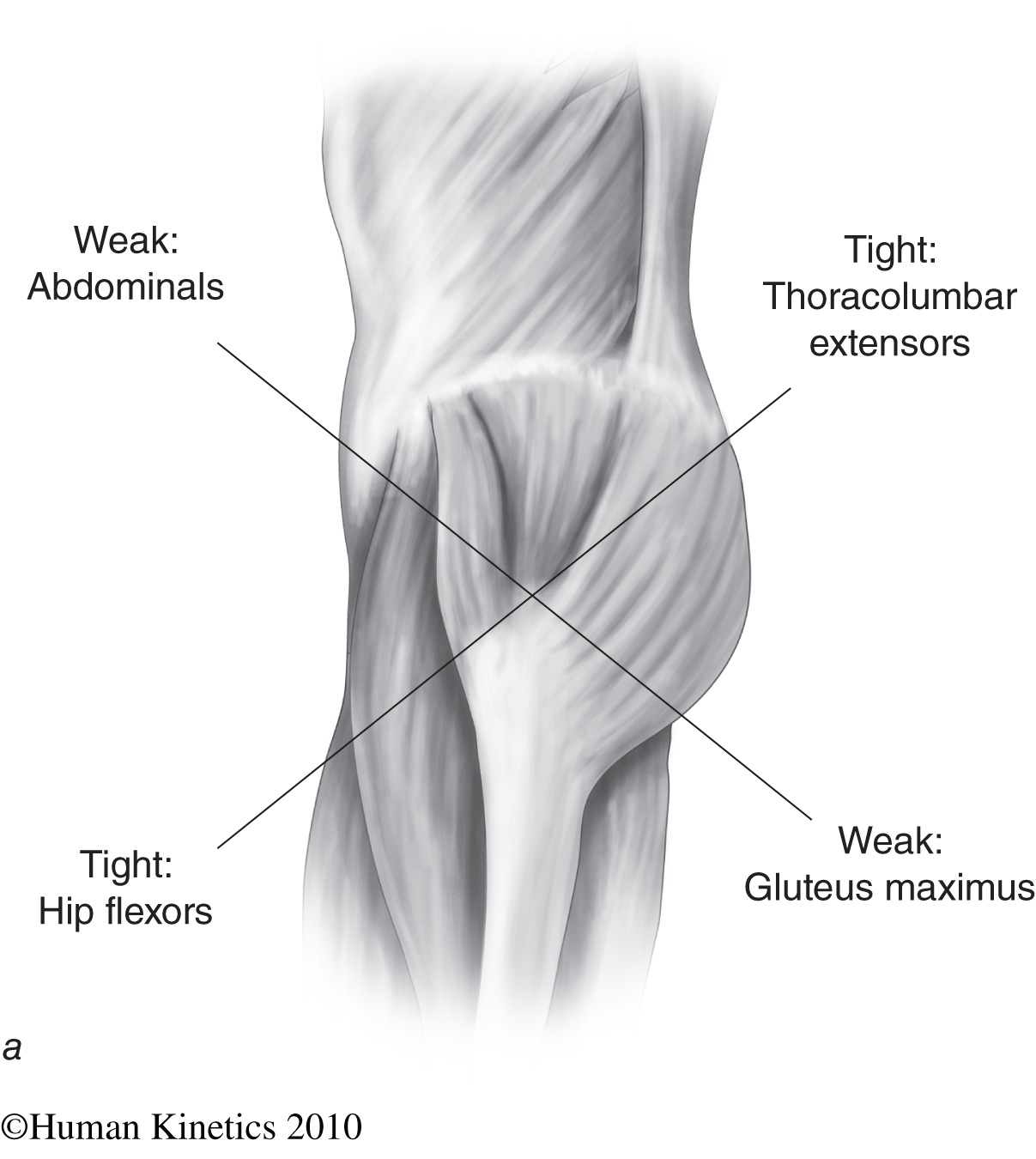
After describing this method of looking at compensation patterns, I want to go back to lower cross syndrome. Lower cross syndrome (pictured below) is a pattern of clinical symptoms that consist of tight musculature on one line of the “X” and weak musculature on the other line. The primary hip flexor, the psoas (the bottom left of the “X”) is deeply connected through fascial connections to the diaphragm. Bad posture, sitting in a flexed position for an extended period of time, even stress can cause us to decrease activation of the diaphragm. This is the first step in a potentially large cascade of neurological changes in our body (it’s all about the nerves) that result in compensation patterns. When the diaphragm is restricted, the psoas will also tighten down. Tightness in muscle A leads to down-regulation of its antagonist, muscle B. In this case, tightness in the psoas leads to down-regulation of the glutes (the bottom right of the “X”). If the glutes are down-regulated and unable to perform their primary function of hip extension, the lower back or the hamstrings will pick up the slack to achieve the movement goal of hip extension (think of the string). Now the lower back is having to do two jobs causing tightness within the muscle (the top right of the “X”). Meanwhile on the anterior aspect of the body, the tight psoas and tight lower back leads to an anterior tilt of the pelvis putting the abdominals in a poor position giving a semblance of weakness.
Now let’s apply the joint-by-joint approach presented by Mike Boyle to describe compensation that exists in lower cross syndrome. According to Boyle, joints in the body alternate their movement capabilities and purpose from mobile to stable to mobile and so on. Starting with the ankle as a mobile joint, the knee is a stable joint, the hip is mobile, the lumbar spine is stable, etc. Generally speaking, stable joints move in a single plane whereas mobile joints move in multiple planes. Going off the muscular compensation previously described, if the psoas is tight and the glutes don’t want to work the once mobile hip becomes more stable. Forcing the lumbar spine to become more mobile when trying to accomplish movement goals. Between tight lower back muscles and a lumbar spine having to move more than it should, it’s no wonder why low back pain is such a common complaint. I began describing this compensation pattern with the diaphragm not firing properly, but really compensations can begin at any point along this cascading cycle. Lower cross syndrome is easy to analyze because it exists at the center of the body, these compensations get more complicated the further from center they extend.
The next question is simple, now what? This combination of approaches is how I visualize and deal with muscular compensations. So when an athlete comes to me with quad tightness, I will address the “tight” tissue but I will also check to make sure his hip is appropriately mobile and the muscles around it are able to do their job properly. Because as we’ve discussed, if the psoas isn’t working right the quad will compensate and need to work harder with both hip flexion and knee extension.
One thing I do not understand is why the body is seemingly unable to self-correct these patterns? Somebody who is compensating will continue to use that pattern until they are corrected by some sort of intervention despite the fact that all healthy individuals first learn how to move using the most efficient motor patterns as infants. How prevalent do you think compensation patterns are? Does this model I’ve presented fit your clinical experience? What are some other approaches you all use to identify and treat compensation?
Happy Holidays! I hope you get to take a moment away from the craziness of working in athletics and spend time with family and loved ones. I will see you again in the new year!!
Mark D.
@MarkDomATC

Comments
Post a Comment